


TL;DR
About a year ago, I was diagnosed with testicular cancer. About a week ago, my CT scans still showed no signs of metastasis. That’s great, and my general experience up to now was as pleasant as possible. This post is to provide other graduate students with the inside experience of being diagnosed with cancer during your PhD, and to highlight some of the issues I’ve noticed along the way. Most importantly, students with serious illnesses generally aren’t supported very well by their grant, cancer has some unexpected mental side-effects, and people should stop referring to it as a ‘fight’.
Disclaimer: This is my story; your experience may differ.
Diagnosis
To put it bluntly, I woke up with a nasty ache in my nuts one day. It didn’t subside during the day (cycling to work didn’t help!), so I scheduled an appointment with my GP. The next day, the pain got worse, and I phoned the doctor’s office to ask whether I could come in directly. At this point, my testicle was about the size of a chicken egg, and I was genuinely concerned.
The first time someone other than a romantic partner asks you to pull down your trousers is a bit weird. Even more so in this case, as a medical student was present: This guy was of my age and went to my university, and was now examining my testicles. What’s interesting, though, is how quick the initial weirdness fades. Medical professionals see these things all the time, and your junk isn’t going to be very different from somebody else’s. No big deal. At this point, the number of people who have touched my genitals for medical reasons is greater than the number of people that have touched them for recreational purposes. I realise that the idea of a stranger seeing and examining your crown jewels can put men off seeing their doctor, but seriously, take it from an experienced patient: Go see your GP if you think something is amiss.
In my case, the doctor pointed out to me and his student, that my giant ball was likely caused by an infection-related build-up of fluids. He prescribed some antibiotics, and asked me to come back in two weeks. The course of antibiotics removed the pain, but didn’t decrease the swelling. So after re-examining my chicken egg, the GP referred me to a urologist. You should know that testicular cancer is really incredibly rare: the incidence in Western countries is only between 1 and 8 people in 100 000 [1], although it does seem to be on the rise [2]. So it’s completely reasonable that my GP initially thought of something else.
After seeing an ultrasound scan of my scrotum, the urologists first words were “Well, there’s no easy way of saying this: You have cancer.” I appreciated his frankness, but was too flabbergasted to fully appreciate the gravity of what he had said. Of course, I had spent some time Googling the potential causes of suddenly increased trouser-bulges. My conclusion had been that cancer would be very unlikely, and I even felt comfortable enough to joke about it. The urologist explained the biology behind testicular cancer, and briefly went over what the next few weeks would bring. My only real concern was with the survival rate, and I vaguely recall asking about it several times. Pro-tip: Bring a notebook to every doctor’s appointment, because retaining information is incredibly challenging in these situations.
The urologist left me with a wonderful specialist uro-oncology nurse, who explained to me that there would be blood tests, an operation, more blood tests and a CT scan, and that we would only really know how serious the cancer was after the results of those tests were in. This is where the first mental challenge starts: You’ve just been told you have cancer, but you won’t know whether it has spread throughout your body until several weeks from now. The suspense is terrible.

Penis-shaped liquorice from the Netherlands, bitten into my post-operative shape.
Finding your way through cancer
The treatment of testicular cancer is very stereotyped: An operation is performed to remove the affected testicle, a biopsy is performed on the removed tumour to establish what type of cancer you have, and a CT scan of your abdomen and chest should show how far the cancer has spread. If the cancer has spread, you receive several courses of chemotherapy. How many courses and what type of chemo depends on the type of tumour. In general, the survival rates are high. Testicular cancer is the lighting example in oncology, because platinum-based chemotherapy has greatly increased the likelihood of surviving, and curing patients is now actually a realistic possibility. That’s your tax and charity money at work!
As a newly-diagnosed patient, you read about this information on all sorts of leaflets and websites, but all you think is “OH MY GOD, I’M SURE I HAVE THE WORST CANCER EVER, AND I’M GOING TO DIE!“. At least, that’s what I thought, and I’ve since learned that this is a very common response. If you’re reading this because you’re in a similar situation, I would strongly recommend joining MacMillan’s Online Community, where patients and other affected people (friends/family) can exchange experiences and information. There are communities for almost every type of cancer, and they are a great place to ask all your questions, and to talk about your fears and anxieties about what’s to come. If you Google stuff, you will browse through websites until you find one that tells you that you are likely to die. If you ask about the same thing on the support forum, you usually receive more up-to-date and realistic information.
Although you initially greatly over-estimate the chance that your disease will kill you, there is no denying that it is a possibility. Especially when you’re young, that’s not a pleasant realisation. Coping with your mortality is a very personal experience, and I don’t think there is a perfect way of doing it. For me, complete and utter nihilism actually really helped. Imagine the universe a billion years from now. You’re not in it, your loved ones aren’t in it, and even your planet isn’t in it. Heck, at some point, not even warmth will be in the universe anymore. The inevitability of this outcome makes whatever you do completely futile. On a smaller scale, you will cease to exist when your brain dies. That means you won’t be able to think about anything anymore, nor relive any memory. Once you’re dead, that’s it for you. So it doesn’t matter how and how long you’ve lived; at the end of it, it will be reduced to nothing anyway. To me, that’s not depressing, it’s liberating. I don’t have to create a legacy (there won’t be any left at some point), and I don’t have to be too concerned with the future (it’ll end anyway), so I can spend my days doing whatever.
Before anything was done to me, I was advised to store some sperm. Cutting out one of your testicles doesn’t necessarily render you infertile, but chemotherapy will. Usually, your fertility will recover, but there is a chance it will be gone forever. Storing sperm is a surreal experience. You’re asked about what you’d like to happen to your deposit in the event of your death. Are you comfortable enough for your partner to use it if you die? And what is your long-term plan, in the event you live long enough to produce offspring? Will it be possible to transport the stored sperm to a different facility, even when that is in a different country? (Yes!) And how much does it cost? (Around 200-300 pounds a year.) After having that conversation, you’re led into a room that is somehow exactly like you expect it to be. Leather couch with metal accents, dirty magazines in a corner, tissues everywhere. The following pictures tell the whole story, really. Walking into this room was the first time I laughed since the diagnosis three days earlier.

This is an actual room in a sperm storage facility.
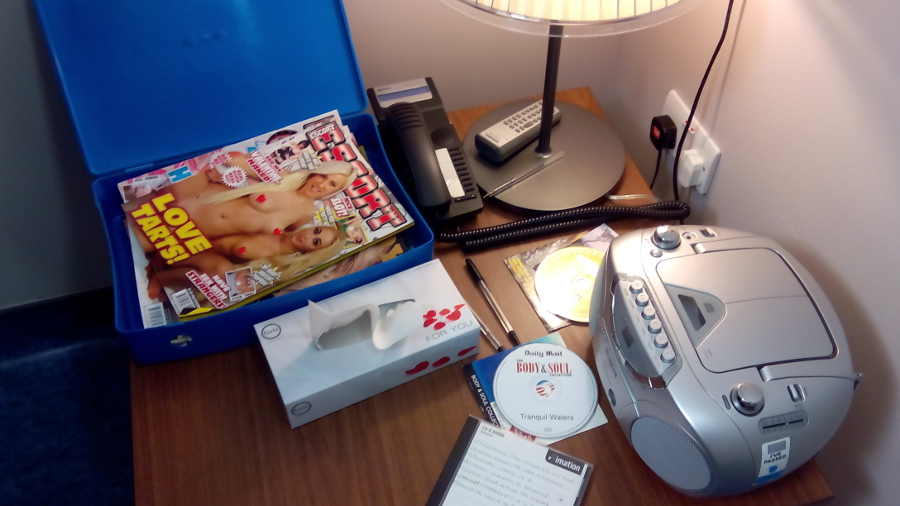
These are actual magazines in a sperm storage facility.
The actual operation, an orchiectomy, isn’t too bad. An incision is made in the groin (much like with a hernia), the blood and lymph vessels in spermatic cord are clamped (to prevent bits of the tumour from spreading during surgery), and I imagine the testicle is pulled and pushed out. Urologists have to do a certain number of these procedures per year to be allowed to do them, so they will be competent. The whole things takes less than an hour, and you are usually allowed to go home on the same day. Unfortunately, I wasn’t, because my operation happened in the early evening (late schedule, running even later). The upside of this was that hospital food tasted great after not eating for a day!
Staying on a ward is weird, though. All other patients were worse off than me, and made noises of agony. There was also a demented patient down the hall, who was probably scared and disoriented. He screamed throughout the night, and fought the nurses. Even after being there for just one night, I’ve gained a lot of respect for them. They do an amazing job in very difficult circumstances.
Some random advice for fellow patients: You will spend a lot of time waiting around. Bring a book, but be careful about which one. I read On the Move, Oliver Sacks’ autobiography, and that was a mistake. Don’t get me wrong, the book is great. But a few pages in, Sacks describes that when he was a pre-med student, a fellow Oxford student (like myself) came to him with a medical issue. His testicle had swollen to the size of an egg (like mine). Sacks told the guy that he might have testicular cancer (again, like me!), and that he should visit a doctor. Turns out he did have cancer, and died soon after (F*CK, THAT COULD BE ME!). It doesn’t end there, as a lot more people die of cancer in that book. Not very uplifting to read, if you’re still unsure about your own faith.
I was lucky: There were no signs of metastasis in my biopsy or my post-op CT scan. My blood levels also returned to normal. That does not mean it’s all hunky-dory; it could be the cancer has spread, but that it’s not detectable on scans or in the blood yet. That’s a terrifying thought, and I’ll return to that later. For now, the oncologists advised me to go on a surveillance trajectory. When the cancer does show up, they can always start chemo. If it doesn’t, then there’s no need for future treatment. Chemotherapy has many nasty side-effects, including death by infection during the treatment, and also an elevation of your chances of getting more cancers. Avoiding it when it’s not necessary is best.
As a final note on the treatment, I would like to add that the ‘fighting’ metaphor for dealing with cancer is awful. I get that it’s appealing, as it can make you feel as though you (or your loved one) has some control. But, unfortunately, it doesn’t work like that. You don’t ‘fight’ cancer. You suffer from a stochastic and massively complex process, and whether you make it through isn’t up to you. It is in some way, as you choose to adhere to your treatment regime or not, but you won’t overturn your cancer by wanting it real bad. Keeping your chin up and being positive is great, and has been shown to be relate to how you will feel throughout and after your illness [3]. But the downside of the fighting metaphor, is that it inherently suggests that you can ‘lose’ if you didn’t fight enough. That’s simply not true: Very strong people die of cancer, and none of them by fighting too little. As an alternative, I love how Maggie’s Centres phrase it on their information posters: “Finding your way through cancer“. This is much truer to what the actual process is like, whether it ends in death or not.
In remission?
So, you’ve had an operation, probably chemotherapy, and your test results come back negative. Are you out of the woods now? People ask this regularly, and the answer is more complex than you might think. In fact, you just don’t know. Before the operation, some cancerous cells might have spread to other parts of your body. These cells can start to form secondary tumours where they land. Initially, these tumours will not be large enough to show up on CT scans, and they won’t produce enough tumour markers for blood tests to pick up. How quickly these secondary tumours grow depends on what their surroundings are like. If they don’t have a good food supply, it can take years for them to slowly grow large enough to show up. So most patients in remission could have a little tumour growing in them, just waiting to rear it’s ugly head.
Randall Munroe catches this feeling really well in his xkcd comic ‘Lanes’ (also included below). Knowing that something might still be growing inside of you can be rather disturbing, as this video clearly illustrates. This is another major mental challenge, as it can make you incredibly sensitive to potential symptoms. Abdominal pain? It’s probably spread to your lymphs there. A cough? Yep, it’s in your lungs now. Swollen lymph nodes in your neck? Oh, no, it’s in your neck; so it’s probably also in your brain now.
I was never a hypochondriac. In fact, before my testicular issues, I had only been to the GP twice in my adult life. Since being diagnosed with cancer, I involuntarily pay more attention to my body. If something feels amiss, I immediately think “Oh, no, it has spread”, often before I’m even fully aware of the actual issue. It takes a conscious effort to suppress this kind of thinking. In addition, I’ve learned that knowing about psychosomatic processes does not make you immune to them. When I worry about abdominal or neck lymphs, I’ll have abdominal or neck pains soon after. I know that I’m imagining things, but that doesn’t stop it from happening. The mind is a powerful thing, and it’s fascinating to witness these processes from a patient perspective.
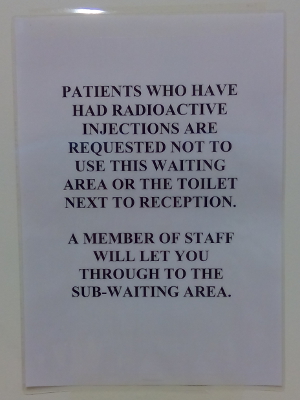
No peeing if you’re radioactive!
Academic consequences
As a PhD student, I have three years to finish my thesis. In order to do this, I need to do research: conduct experiments, analyse my data, write up my results; rinse and repeat. Three years is a short time to produce a lot of good work, especially since a large part of every PhD is learning all sorts of new techniques (handling specific equipment, analysing data with certain methods, programming, and so on). PhD students are part of a university department, and they are supervised by a senior academic. The experience is very similar to being a junior employee in any other job. Despite working full-time (and often more) and doing a lot of work for the department, PhD students are not normally considered to be an employee. Instead, they are students who receive a stipend instead of a salary.
Having a student status does not only mean you earn less money than your working peers do, it also means you have less rights. If everything goes along smoothly, that is no issue: It’s good fun to be expected to act as a student a bit longer, and you can do good work even without having a decent employment contract. However, when a graduate student is faced by a serious illness, things start to break down. This is painfully apparent in the Grant Terms and Conditions from Research Councils UK [4]. Clause 58 reads “The Research Organisation must make suitable arrangements for coping with absences of students for illness, maternity leave, Ordinary Paternity Leave, shared parental Leave, adoption leave, extended jury service and holidays“. This points to the university to make arrangements for ill students. However, these illnesses are only expected to be 13 weeks or less. Clause 60: “Payment of a studentship can continue for absences covered by a medical certificate for up to thirteen weeks within any 12-month period. If the illness lasts, or is expected to last, for more than thirteen weeks, the Research Organisation should make arrangements to suspend the studentship“.
So if you have cancer and require surgery and chemotherapy, your stipend is likely to be suspended. The same regulations also discourage other employment: clause 38 forbids full-time employment, and points out that part-time employed students are only eligible for part-time awards. This means that their stipend is most likely a PhD student’s only livelihood. Having that suspended because you’re seriously ill, means that you need serious financial reserves, or face being homeless and hungry.
To put this in perspective: PhD students are typically in their mid-twenties or early thirties, and academic peers with a staff contract are allowed up to 6 months of paid sick leave. I was one of those lucky bastards, as my grant comes from the European Commission’s Marie Sklodowska-Curie programme. This requires the university to sign PhD students onto a staff contract. Thanks, EU!
I don’t have to point out that suspending PhD students’ livelihood when they get cancer or any other serious illness is not OK. Research Councils in the UK, and equivalent funding sources elsewhere, should revise their rules.
Acknowledgement
I thought about acknowledging all the wonderful people who have helped and supported me during the past year, but I decided against it. Not because I’m ungrateful, but because I can’t fit the names of all those people that I’m grateful to on here. You’re all the best.
There is one person I would like to mention by name, and that is Rabea Nourbakhsh. She is the mother of a friend and colleague of mine, and she was diagnosed with brain cancer a little over a year ago. Although I never met her, I felt connected through our diseases, through her daughter, who was an amazing support to her and to me. (Your green drinks tasted so awful, they must have been super healthy!) Sadly, Rabea suffered from a very aggressive brain tumour, and she passed away recently. The reason I mention her by name here, is that her amazing family are honouring her last plans to raise money for the medical aid of refugees in the Middle East. Her website is in-her-memory.com, if you’d like to know more.
References
- Adami et al. (1994). Testicular cancer in nine northern european countries. International Journal of Cancer, 59(1), p. 33-38. doi: 10.1002/ijc.2910590108
- Huyghe et al. (2003). Increasing Incidence of Testicular Cancer Worldwide: A Review. Journal of Urology, 170(1), p. 5-11. doi: 10.1097/01.ju.0000053866.68623.da
- Spiegel, D. (1997). Psychosocial aspects of breast cancer treatment. In Seminars in Oncology-Supplements (Vol. 24, No. 1, pp. 36-47). New York, USA: Grune & Stratton.
- Research Councils UK (2014). Conditions of Research Council Training Grounds. Retrieved from: www.rcuk.ac.uk/funding/grantstcs. Click here for a PDF version.
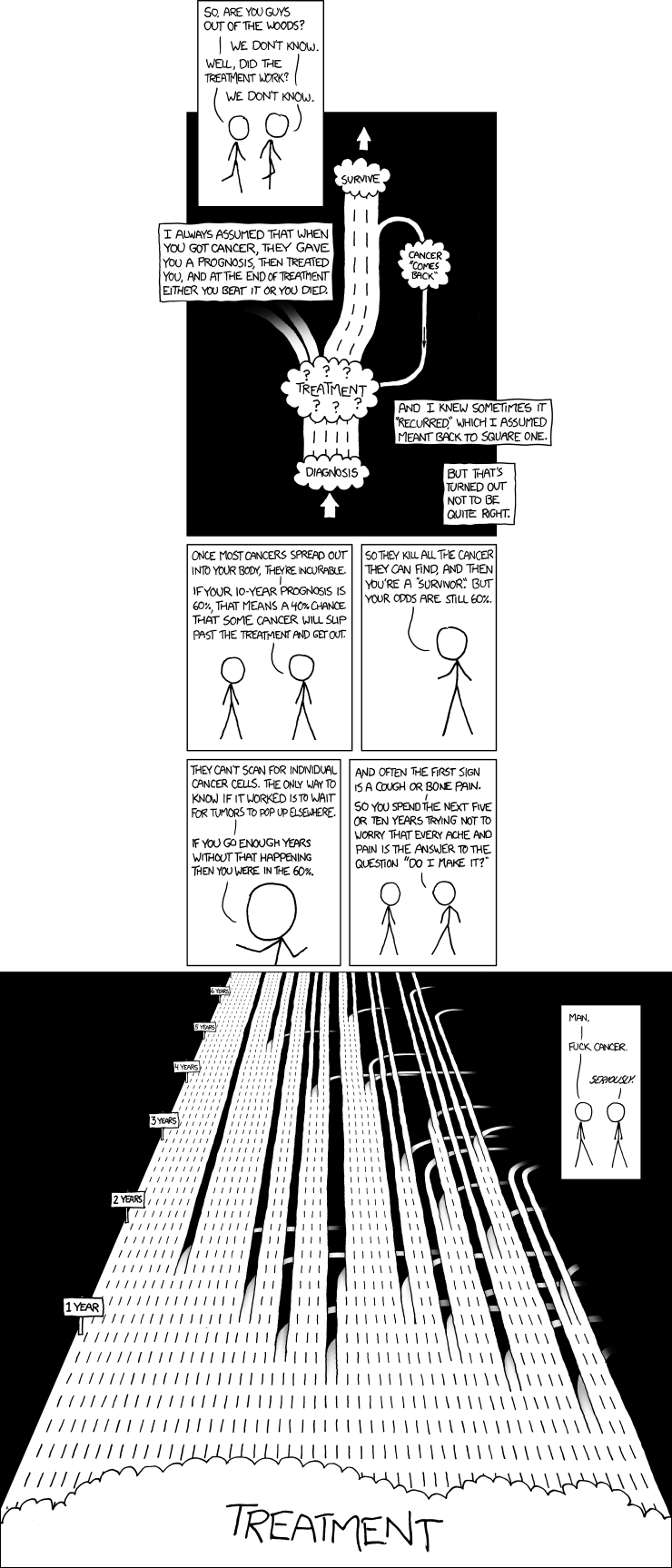
Randall Munroe’s comic ‘Lanes’ (xkcd nr. 931). From: xkcd.com/931
Hey Edwin. Came to your site for the Gmail Auto Responder script, trying to get sodding Gmail to auto reply an email, suddenly stopped working then took me an hour to figure out it stops automatically once you’ve reached your run limit – I was mad. Then this story caught my eye, needless to say a stupid email redirection problem or any other non life-threatening issue is nothing when hit with a serious condition…..Makes one remember the important things in life.
Thanks for shaving and I wish you all the best for the future…..
Hi Peter, Thanks for your message!
As for the Gmail issue: I’m quite impressed that you managed to hit the Google’s limits. Or was it a Google Script issue? Either way, hope you get it sorted!
Hello Edwin,
I came across this website because I was doing some online digging on eye-tracker softwares and image processing (to help with my bachelor’s thesis), and consequently read this blog of yours.
Cancer sucks, period. I remember this one time that my GP found a lump in my breast and I needed to get that checked out. I was scared shitless the whole time. Since it didn’t turn out to be cancerous, I guess I can’t really say that I understand what you must have experienced, but you have my sympathy.
I loved the humourous tone in the entire post, even though it was about something serious. I hope you kick cancer’s ass (or nuts, whichever you prefer)
Thanks for your message! I’m glad you appreciated the post, and even gladder that your lump wasn’t cancerous Hope you found what you were looking for on the eye tracking. If not, the PyGaze forum a good place to ask questions: http://forum.cogsci.nl/index.php?p=/categories/pygaze
Hope you found what you were looking for on the eye tracking. If not, the PyGaze forum a good place to ask questions: http://forum.cogsci.nl/index.php?p=/categories/pygaze
Hi Edwin,
Just happened upon your post through random googling, and really appreciate everything you’ve written here. I identify with this SO MUCH. Although I don’t have cancer, I’m a PhD student in the humanities, and I have lupus and severe asthma. I just started immunosuppressant therapy for my lupus, which is akin to low-dose chemo. Though most people with lupus will have a normal lifespan, there’s similarly no doubt that people do die from this disease and can have a lower quality of life because of possible organ involvement, including reduced kidney function.
Unfortunately, here in Amurika, grad students have even fewer rights than the Research Council seems to grant you, and our degrees take twice as long because we’re also expected to fulfill teaching responsibilities… We have no paid leave at all and no access to disability benefits either because we aren’t technically considered “employees.” I’ve been without a stipend now for months, and was cut off from my university health insurance because it’s their policy that you can only be covered during the first semester that you’re on leave. I’m now paying for private coverage and have had to rely on my family for financial support.
Anyway, I don’t really know what this comment is accomplishing other than to say YES, SAME (SORT OF) and thank you for speaking out. I agree that illnesses shouldn’t be referred to as battles. The same “battle/survivor” mumbo-jumbo is bandied about with equal ridiculousness about lupus, which is silly because no one actually knows whether or not they have truly “beaten” the disease. It’s all about embracing the unknown.
Hi Holly,
So sorry to hear about your illness, but thanks for speaking out too! It sounds like the situation in the US is even worse, and that really sucks. It’s such an idiotic and cruel system, where we’re essentially being punished for falling ill. We’re adults who work full-time jobs; how come we can’t have the same rights as other adults doing full-time jobs?
I hope that your situation improves, and that you can manage to cope with your condition! Don’t hesitate to reach out if you need some kind of support (That goes for everyone reading this, BTW!)
(That goes for everyone reading this, BTW!)
Cheers,
Edwin
Hey Holly
We are running a network of disabled academics called chronically academic.
Perhaps one of our members knows a source of funding (I mean, we have people with such problems, and they managed to resolve them somehow – if you want to get in touch with us, we could think of a solution together)?
Maria
Pingback: Friday links: Freeman Dyson vs. community ecology, “white trash” in academia, and more | Dynamic Ecology
I’ve just randomly found this post. You’ve reflected similar experiences to mine. I had a kidney tumour shortly before neuroscience exams – all the uncertainty around diagnosis and pre-op, and post-op recovery) was indescribably hideous. I’d had breast cancer 10 years before; I was told I had liver secondaries, while writing up my final year undergrad project!
I’m not sure how I got through those exams and project; how did you get through your work?
I see you’ve a book out on Python – maybe you’ll write a book on your experiences with cancer!
Wow, two separate tumour diagnoses? That’s rough! Hope you’re doing well?
To be honest, I doubt whether my experience is worthy of a book at all. I got away relatively easy, or at least it’s currently looking that way. Single tumour, no metastasis as of yet, and a young and otherwise healthy body to cope with the surgery. But to answer your question:
For me, work was a nice distraction in the very uncertain weeks after the diagnosis. For all I knew, the cancer could have spread out everywhere, and that was a very scary thought. In addition, after the operation, I couldn’t really go anywhere (groin incision, so walking is out of the question for a week or two; let alone cycling!). So I was stuck at home with plenty of time to worry about what might happen. Instead of worrying, I prepared for my transfer of status by analysing some data and writing up the report. (This is a thing you have to do at the end of your first PhD year, on the basis of which the university decides whether they trust you to actually finish your PhD. You have to pass to be allowed to go on.) So my work really helped to distract me from the diagnosis.
The diagnosis also helped me with work. It made it very clear what was and wasn’t important, and it put an extra time pressure on my PhD work. I ended up focusing more on my own work, and to stop some collaborations with others. Luckily, those colleagues understood the situation, and were happy to find alternative ways of getting the work done.
I enjoyed your post very much, thank you – very honest, which I appreciate. I’ve booked marked it as I feel I’m going to come back to this from time to time. I’m currently at the write up stage of my PhD and in three weeks time I’m due to start a full time, permanent lecturer post – fab right?! The slight spanner in the works is two days ago I was diagnosed with breast cancer and due to have a mastectomy in just under two weeks time. The rest of the treatment is unknown at this stage. The day I was told, I was a mess as I really wasn’t expecting it. The day after and today I’ve felt almost normal. Trying to still write at the moment, although it isn’t quite happening! I really want, as much as possible anyway, to hold onto normality. I’m going to try to continue with work and writing up, but only time will tell how it’s all going to affect me. Anyway, cheers for sharing your experience – I really think it helps people. I’m taking each day and each step of the process as it comes!
Pingback: What colleges must do to promote mental health for graduate students | Iranians Global Network
Pingback: What Colleges Must Do To Promote Mental Health For Graduate Students | The University Network
Hi Edwin,
I found this site by typing in “doing a PhD while dealing with cancer” because that’s where I’m at now. Breast cancer – surgery, radiation done and now figuring out the long term meds (the worst part, I think) now. I know lots of people who have (had) cancer, but none while doing a PhD. As an ADHD’er, I already have cognitive challenges and in Japan where I study, Ritalin is no longer allowed as a treatment for ADD/ADHD. But cancer & the treatment seemingly has turned my brain to mush. I was wondering how you’re coping with that. Oddly, I’m studying in the radiology department, so you’d think the profs’d have a clue. But they’re quite puzzled as to why I’m not working at full speed! I don’t have to worry about losing a stipend as I don’t have one, and I can switch around some of my part-time teaching hours (all at different unis) as needed. But the threat of losing income is scary indeed. Anyway, I’m glad to hear you’re in remission, and even though some commenters are also dealing with cancer, if nothing else, I feel less ‘alone’. BTW, love the comics – Yes, “F” Cancer!
Hi Suzy,
Really sorry to hear about your breast cancer. It’s good to hear you feel less alone, though. So F’d upped that your radiology professors have so little understanding for your situation! I do think cognitive fatigue is very common in your situation, and you definitely shouldn’t feel like it’s weird.
Not sure about what to do about your Ritalin. Is Concerta still available? Or any other methylphenidate-based drug? (I’m not sure what the available brands are in Japan, or if they’re even available given the ban you mention.)
Good luck with your PhD and your recovery. I’m rooting for you!
Hi Edwin,
This reply is late, but as the last post before mine was almost 2 years ago, I didn’t expect such a quick reply from you!! Thanks for the well-wishes!. I must apologize (the US spelling…), I hadn’t meant to ask about ADD, just the cancer-brain stuff (see? mush for brains.) Actually, I’ve been to Ireland a few times for conferences & found a doc who prescribes a different (& sadly less effective) medicine which isn’t available in Japan (but not illegal…) The problem is, for the pre-op medical work-up, I figured I’d have to explain it or go off it. Easier to go off it. But I will go back on it very soon as I don’t like walking in circles as if I had rabies LOL! (& yes, I’ve done the research, there’s no interaction with the cancer meds.)
Sometime soon, I’ll head over to the MacMillan site you mentioned in your post. As job security is …tricky, few people know about my cancer. (Luckily, my partner is wonderfully supportive, he’s such a good guy.) Like-minded conversations sound like a good idea. Research articles aren’t all that empathetic!
And one last thing, your post was in 2016 – just curious, have you finished your PhD? (if yes, major congrats!) Were your profs supportive? Did you find a good position? If not yet, are you able to move towards finishing? HAGD!
Hi Suzy,
YES, research papers can be very tough to read without any humans nearby. I really appreciated having direct access to research on treatments and prognoses, and in some ways it made me much calmer about the whole thing, but in other ways it can spark anxiety (e.g. when not knowing your specifics yet, and reading about stage 4 survival rates). Really happy to hear you have a supportive partner! Hope you also found some people who are going through a similar illness via that forum, if that is something that is useful to you.
I did finish my PhD! (See elsewhere on this website for a short blog on it.) I was very lucky with my supervisor, who was amazing and super supportive. He’s just a lovely person in general, but it might also have helped that he’s a neurologist. Found a great postdoc afterwards, which will run for another two years
Hope things are going well on your end!
Pingback: "What Colleges Must Do to Promote Mental Health for Graduate Students" - Ami Axomiya
Pingback: What Schools Should Do to Promote Psychological Well being for Graduate College students - Jobeas
Pingback: "What Colleges Must Do to Promote Mental Health for Graduate Students" - World Of Jobs